- Sep 23, 2005
- 32,043
- 5,868
- Country
- United States
- Faith
- Christian
- Marital Status
- Married
------------Procedural note----------------
Please note this is a focused topic for discussion of prior infection and natural immunity in the context of vaccine mandates. There are many threads already regarding the effectiveness, safety, etc. of vaccines. Please take discussion of safety or efficacy of vaccines, etc. outside of that context to another thread.
------------------------------------------------
There is research showing that natural immunity to COVID 19 in previously infected people is in most cases effective and long lasting (see below for studies).
In light of this, natural immunity should be taken into account when creating vaccine mandates. If someone can demonstrate the presence of antibodies (guidelines could be formed to reduce false positives, through multiple tests, etc.) then this should suffice for vaccine mandates.
A number of those who are reluctant to receive vaccination have already been infected. If they have immunity largely on-par with or surpassing that of vaccinated individuals, then they should not be compelled to take a vaccine.
We are facing worker shortages in the marketplace across various fields currently. Vaccine mandates, whether employer based or government based, could further impact available workers if some decide to resign rather than be vaccinated. Since prior infection with demonstrable antibodies provides effective protection it does not make sense to take these workers out of positions they are currently occupying.
Data also indicates that there can be even greater protection for those who are infected and still get a dose of the vaccine. However, reinfection rates are low with or without the additional dose. And some research indicates increased adverse reactions when those with prior infection receive the vaccine. This is one reason some health care workers with prior infection are reluctant to take on additional risk for quite low improvement in protection afforded by natural immunity:
------
A health system in Michigan has now included prior infection natural immunity in their medical exemptions.
Natural Immunity Vaccine Exemption Now Offered At Spectrum Health
Lehigh Valley Health network has also done so:
St. Luke’s and LVHN employees who caught COVID-19 to defer getting the vaccine, other employers may follow
George Mason University allowed a professor a medical exemption based on this as well.
George Mason relents, grants COVID-19 medical exemption to professor |
----------
A Systematic Review of the Protective Effect of Prior SARS-CoV-2 Infection on Repeat Infection
SAGE Journals: Your gateway to world-class research journals
We systematically reviewed studies to estimate the risk of SARS-CoV-2 reinfection among those previously infected with SARS-CoV-2.
Of those, 10 studies were eligible for our systematic review. The weighted average risk reduction against reinfection was 90.4% with a standard deviation of 7.7% (p-value: <0.01). Protection against SARS-CoV-2 reinfection was observed for up to 10 months.
The protective effect of prior SARS-CoV-2 infection on re-infection is high and similar to the protective effect of vaccination. More research is needed to characterize the duration of protection and the impact of different SARS-CoV-2 variants.
https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full.pdf
This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.
AAAS
The research impresses Nussenzweig and other scientists who have reviewed a preprint of the results, posted yesterday on medRxiv. “It’s a textbook example of how natural immunity is really better than vaccination,” says Charlotte Thålin, a physician and immunology researcher at Danderyd Hospital and the Karolinska Institute who studies the immune responses to SARS-CoV-2. “To my knowledge, it’s the first time [this] has really been shown in the context of COVID-19.”
Necessity of COVID-19 vaccination in previously infected individuals
Summary Cumulative incidence of COVID-19 was examined among 52238 employees in an American healthcare system. COVID-19 did not occur in anyone over the five months of the study among 2579 individuals previously infected with COVID-19, including 1359 who did not take the vaccine.
Lancet
This study supports the hypothesis that primary infection with SARS-CoV-2 provides a high degree of immunity to repeat infection in the short to medium term; with similar levels of prevention of symptomatic infection as the new licenced vaccines for working-age adults. We have also shown that immunity from previous infection is protective against reinfection with the B.1.1.7 variant. Primary infection also reduces the risk of asymptomatic infection and thus onward transmission; this is particularly important as health care was considered a potential driver for ongoing community transmission during the first wave in the UK
A long-term perspective on immunity to COVID
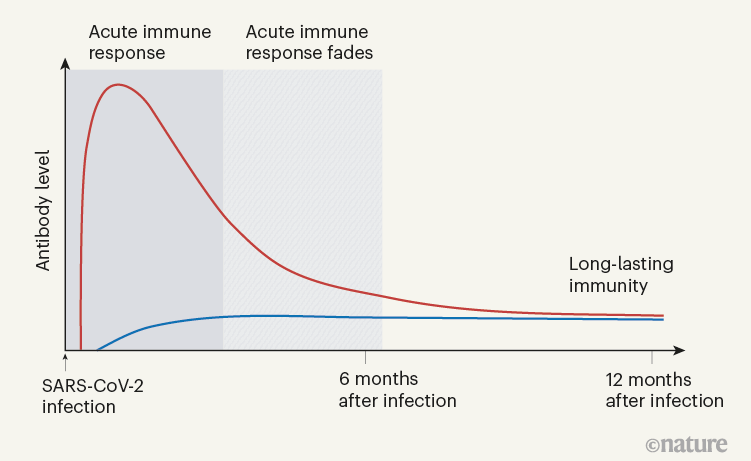
When Turner et al. tracked the concentrations of antibodies against SARS-CoV-2 in the individuals’ blood serum for up to one year, they observed a biphasic pattern (Fig. 1). In the acute immune response around the time of initial infection, antibody concentrations were high. They subsequently declined, as expected, because most of the plasma cells of an acute immune response are short-lived. After a few months, the antibody concentrations levelled off and remained more or less constant at roughly 10–20% of the maximum concentration observed. This is consistent with the expectation that 10–20% of the plasma cells in an acute immune reaction become memory plasma cells5, and is a clear indication of a shift from antibody production by short-lived plasma cells to antibody production by memory plasma cells. This is not unexpected, given that immune memory to many viruses and vaccines is stable over decades, if not for a lifetime8.
Vaccinating people who have had covid-19: why doesn’t natural immunity count in the US?
A large study in the UK and another that surveyed people internationally found that people with a history of SARS-CoV-2 infection experienced greater rates of side effects after vaccination. Among 2000 people who completed an online survey after vaccination, those with a history of covid-19 were 56% more likely to experience a severe side effect that required hospital care.
-----
CDC:
COVID-19 and Your Health
Cases of reinfection with COVID-19 have been reported, but remain rare.

Additional reading:
Lasting immunity found after recovery from COVID-19.
------
AAAS
Substantial immune memory is generated after COVID-19, involving all four major types of immune memory. About 95% of subjects retained immune memory at ~6 months after infection. Circulating antibody titers were not predictive of T cell memory. Thus, simple serological tests for SARS-CoV-2 antibodies do not reflect the richness and durability of immune memory to SARS-CoV-2. This work expands our understanding of immune memory in humans. These results have implications for protective immunity against SARS-CoV-2 and recurrent COVID-19.
I am editing as the thread goes to add new information.
Please note this is a focused topic for discussion of prior infection and natural immunity in the context of vaccine mandates. There are many threads already regarding the effectiveness, safety, etc. of vaccines. Please take discussion of safety or efficacy of vaccines, etc. outside of that context to another thread.
------------------------------------------------
There is research showing that natural immunity to COVID 19 in previously infected people is in most cases effective and long lasting (see below for studies).
In light of this, natural immunity should be taken into account when creating vaccine mandates. If someone can demonstrate the presence of antibodies (guidelines could be formed to reduce false positives, through multiple tests, etc.) then this should suffice for vaccine mandates.
A number of those who are reluctant to receive vaccination have already been infected. If they have immunity largely on-par with or surpassing that of vaccinated individuals, then they should not be compelled to take a vaccine.
We are facing worker shortages in the marketplace across various fields currently. Vaccine mandates, whether employer based or government based, could further impact available workers if some decide to resign rather than be vaccinated. Since prior infection with demonstrable antibodies provides effective protection it does not make sense to take these workers out of positions they are currently occupying.
Data also indicates that there can be even greater protection for those who are infected and still get a dose of the vaccine. However, reinfection rates are low with or without the additional dose. And some research indicates increased adverse reactions when those with prior infection receive the vaccine. This is one reason some health care workers with prior infection are reluctant to take on additional risk for quite low improvement in protection afforded by natural immunity:
------
A health system in Michigan has now included prior infection natural immunity in their medical exemptions.
Natural Immunity Vaccine Exemption Now Offered At Spectrum Health
Lehigh Valley Health network has also done so:
St. Luke’s and LVHN employees who caught COVID-19 to defer getting the vaccine, other employers may follow
George Mason University allowed a professor a medical exemption based on this as well.
George Mason relents, grants COVID-19 medical exemption to professor |
----------
A Systematic Review of the Protective Effect of Prior SARS-CoV-2 Infection on Repeat Infection
SAGE Journals: Your gateway to world-class research journals
We systematically reviewed studies to estimate the risk of SARS-CoV-2 reinfection among those previously infected with SARS-CoV-2.
Of those, 10 studies were eligible for our systematic review. The weighted average risk reduction against reinfection was 90.4% with a standard deviation of 7.7% (p-value: <0.01). Protection against SARS-CoV-2 reinfection was observed for up to 10 months.
The protective effect of prior SARS-CoV-2 infection on re-infection is high and similar to the protective effect of vaccination. More research is needed to characterize the duration of protection and the impact of different SARS-CoV-2 variants.
https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full.pdf
This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.
AAAS
The research impresses Nussenzweig and other scientists who have reviewed a preprint of the results, posted yesterday on medRxiv. “It’s a textbook example of how natural immunity is really better than vaccination,” says Charlotte Thålin, a physician and immunology researcher at Danderyd Hospital and the Karolinska Institute who studies the immune responses to SARS-CoV-2. “To my knowledge, it’s the first time [this] has really been shown in the context of COVID-19.”
Necessity of COVID-19 vaccination in previously infected individuals
Summary Cumulative incidence of COVID-19 was examined among 52238 employees in an American healthcare system. COVID-19 did not occur in anyone over the five months of the study among 2579 individuals previously infected with COVID-19, including 1359 who did not take the vaccine.
Lancet
This study supports the hypothesis that primary infection with SARS-CoV-2 provides a high degree of immunity to repeat infection in the short to medium term; with similar levels of prevention of symptomatic infection as the new licenced vaccines for working-age adults. We have also shown that immunity from previous infection is protective against reinfection with the B.1.1.7 variant. Primary infection also reduces the risk of asymptomatic infection and thus onward transmission; this is particularly important as health care was considered a potential driver for ongoing community transmission during the first wave in the UK
A long-term perspective on immunity to COVID
When Turner et al. tracked the concentrations of antibodies against SARS-CoV-2 in the individuals’ blood serum for up to one year, they observed a biphasic pattern (Fig. 1). In the acute immune response around the time of initial infection, antibody concentrations were high. They subsequently declined, as expected, because most of the plasma cells of an acute immune response are short-lived. After a few months, the antibody concentrations levelled off and remained more or less constant at roughly 10–20% of the maximum concentration observed. This is consistent with the expectation that 10–20% of the plasma cells in an acute immune reaction become memory plasma cells5, and is a clear indication of a shift from antibody production by short-lived plasma cells to antibody production by memory plasma cells. This is not unexpected, given that immune memory to many viruses and vaccines is stable over decades, if not for a lifetime8.
Vaccinating people who have had covid-19: why doesn’t natural immunity count in the US?
A large study in the UK and another that surveyed people internationally found that people with a history of SARS-CoV-2 infection experienced greater rates of side effects after vaccination. Among 2000 people who completed an online survey after vaccination, those with a history of covid-19 were 56% more likely to experience a severe side effect that required hospital care.
-----
CDC:
COVID-19 and Your Health
Cases of reinfection with COVID-19 have been reported, but remain rare.
Additional reading:
Lasting immunity found after recovery from COVID-19.
------
AAAS
Substantial immune memory is generated after COVID-19, involving all four major types of immune memory. About 95% of subjects retained immune memory at ~6 months after infection. Circulating antibody titers were not predictive of T cell memory. Thus, simple serological tests for SARS-CoV-2 antibodies do not reflect the richness and durability of immune memory to SARS-CoV-2. This work expands our understanding of immune memory in humans. These results have implications for protective immunity against SARS-CoV-2 and recurrent COVID-19.
I am editing as the thread goes to add new information.
Last edited:
